
Why hospital design matters
We are excited to announce that we recently published another article on the topic of stroke rehabilitation and the built environment. Unlike the systematic literature review featured in our last post, this article is designed for a clinical and end-user audience. It has two main areas of focus that are described below: 1. Healthcare built environment research generally, and 2. Stroke specific research. We also discussed the importance of the healthcare design and research process, and produced some key messages in relation to this (listed at the end of this post).
1. Healthcare built environment research
We looked at the range of research on the link between the built environment and healthcare outcomes, and identified stroke, and in-particular sub-acute stroke care and rehabilitation as an area that is in need of more research. Thankfully, this is exactly where NOVELL is working hard to provide evidence and insights. The image below is taken from our article and graphically represents the volume of published research that is focused on different areas of healthcare environments. As you can see, the research covers a broad range of areas, with a significant amount of research looking at the design of Intensive Care Units, Acute Patient Rooms, Emergency Departments, Mental Health Units, and the General Hospital Enviornment. By comparison, acute and subacute rehabilitation have received very little attention to date.
The amount of research that looks specifically at care for people who have had stroke is unsurprisingly a much smaller field, but given the length of time stroke survivors spend in these environments, any improvements in the built environment could have a tremendous impact on recovery.
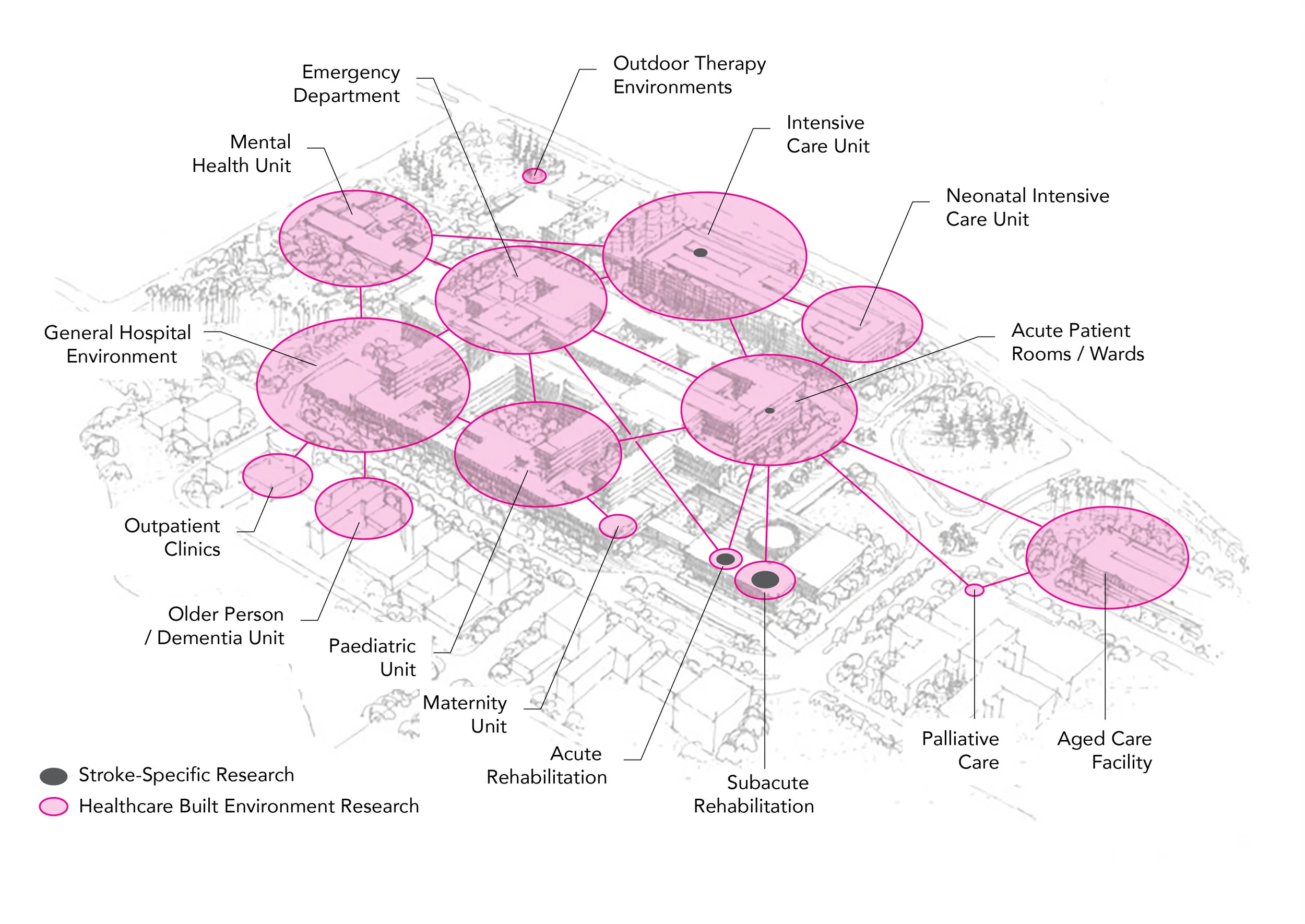
Figure 1. The volume of built environment research conducted in different healthcare settings. Circle size indicates the number of published research articles based on a systematic literature review (in preparation) and articles listed in the Centre for Healthcare Design research repository. Pink circles represent all built environment research, dark grey circles indicate stroke-specific research. (The aerial sketch in the above image has been adapted with permission from Architectus + HDR)
2. Stroke specific research (evidence for rehabilitation design)
The review also zoomed in to these rehabilitation environments specifically, and looked at the amount of evidence we have for making decisions about the built environment in this context. Again, we have represented this graphically so that you (and our clinical audience) can begin to get a sense of the information that is out there. We use the figure below to highlight areas where we have evidence for a connection between factors in the built enviornment (the top row) and stroke survivor outcomes (the bottom row). The strongest evidence is represented with a thick solid line, while weaker evidence is represented with a thinner solid line. Where we assume there is a link between elements, but there is not yet enough stroke-specific evidence to back up this link, this has been connected with a dotted line.

Figure 2. A summary of the evidence specific to stroke care environments. Dotted lines = a hypothesis, garnered from research in other populations; Thin lines = limited evidence, < 3 studies; Thick lines = moderate evidence, ≥ 3 studies, based on systematic literature review (see previous blog post).
The strongest evidence can be found in the link between the built environment and patient social interaction (blue), while we found comparatively less evidence to demonstrate a link between many of the safety and wellbeing measures and the built environment. Many of the dotted lines in this section represent work that has been undertaken in environmental psychology, and in some of the other areas of the hospital described in Figure 1 above.
Key messages
The key messages we hope you, and our clinical audience take from the review are:
We need to work together in interdisciplinary teams (including clinicians) when designing healthcare facilities
We need to promote shared-decision making, collaboration, consultation between architects & healthcare professionals
We should use participatory design, co-design, and Living Labs to involve engaged and informed clinicians in built environment design and research, and
We should make evaluation a priority, freely share what works and what doesn’t, and integrate this into evidence- informed building standards.
You can find out a little more about the paper in the infographic below, or, you can read the full paper. Feel free to also download and share the infographic below with your networks.
